

Translate this page into:
Enamel Demineralization Adjacent to Orthodontic Brackets Bonded with ACTIVA BioACTIVE-RESTORATIVE
This article was originally published by Wolters Kluwer and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction
Enamel demineralization adjacent to orthodontic brackets has been shown to be a consequence during orthodontic treatment. Fluoride-releasing resin-modified glass ionomer cements (RMGICs) have been shown to protect the enamel from white spot lesions, but their bond strength has been proven inadequate. The purpose of this study was to evaluate ACTIVA BioACTIVE-RESTORATIVE, a bioactive material with strength superior to RMGICs, for inhibition of enamel demineralization surrounding orthodontic brackets.
Materials and Methods
Fifteen human teeth were sectioned and divided into two groups. One group was the control and had orthodontic brackets bonded with Transbond XT, while the second group had orthodontic brackets bonded with ACTIVA. The teeth were varnished within 2 mm of the bracket margins and immersed in an artificial caries solution for 3 days to create carious lesions. The teeth were sectioned and viewed under polarized light microscopy for the detection of enamel demineralization adjacent to the bracket, and then, the lesion areas were measured with a computer imaging system.
Results
There was a statistically significant difference (P ≤ 0.001) that ACTIVA had less enamel demineralization adjacent to the bracket when compared to the control group.
Conclusions
The results of this study have demonstrated that ACTIVA, a fluoride-releasing bioactive restorative material, inhibits demineralization of enamel adjacent to orthodontic brackets when compared to a nonfluoride-releasing control.
Keywords
ACTIVA
enamel demineralization
orthodontic brackets
white spot lesions

Introduction
Enamel demineralization adjacent to orthodontic brackets is a risk associated with orthodontic treatment. Orthodontically treated patients have significantly higher risk for developing these white spot lesions (WSLs) than an untreated patient.[1,2] Gorelick et al. reported an increase in WSLs in 50% of patients after orthodontic treatment, and these lesions may develop as early as 4 weeks.[3,4] Risk factors of developing WSLs include treatment time in excess of 36 months, teeth without fluorosis, patients with poor oral hygiene, patients whose oral hygiene declines during treatment, and preexisting WSLs.[5] These risk factors are attributed to the increased plaque around brackets and appliances, change in microflora, and the attachment of the bacteria to the bonding materials. Plaque has been shown to accumulate on brackets and bonding materials, even in participants with good oral hygiene.[6] Excess bonding composite around the bracket base is the critical site of plaque accumulation associated with fixed appliances due to its rough surface texture and the setting shrinkage gap along its periphery.[7] Studies have documented that this increased plaque accumulation in patients undergoing orthodontic treatment shows a significant elevation in the levels of microbial populations, including Candida albicans, mutans streptococci, and Lactobacillus during the course of their treatment.[8-10] It has also been shown that the saliva pH decreases during the span of orthodontic treatment, thereby making the oral environment even more susceptible to demineralization.[10]
Studies have proven that fluoride application can inhibit and prevent the demineralization of enamel.[11-13] Meticulous oral hygiene with daily use of high fluoride toothpaste and a fluoride rinse can also reduce the prevalence and incidence of WSLs.[14,15] However, this proper homecare requires excellent patient cooperation. Fluoride-releasing resin-modified glass ionomer cements (RMGICs) can be used to bond the orthodontic brackets at the initial bonding appointment. The clinical use of fluoride-releasing adhesives has demonstrated significantly smaller enamel lesions when compared to teeth bonded with resin-based composites.[16-21] Although RMGICs have been shown to decrease incidence of WSLs, studies have shown that there is substantially more bond failures that occur with a RMGIC compared with a resin-based composite bonding system.[22] ACTIVA BioACTIVE-RESTORATIVE is a recently introduced enhanced RMGIC, which the manufacturer (Pulpdent Corporation, Watertown, MA, USA) reports to possess the properties of a RMGIC plus a modified resin matrix with improved resilience and physical properties.[23] Although there has not been any studies on the bracket bond strength of ACTIVA, it has demonstrated flexural, compressive, and tensile strength comparable to composites and far superior to glass ionomer cements and RMGICs.[23,24] The purpose of our study was to investigate the inhibition of enamel demineralization surrounding orthodontic brackets when bonding brackets with ACTIVA.
Materials and Methods
Fifteen caries-free human molars and premolars were obtained and debrided of any residual soft tissue. The fifteen teeth were sectioned in half vertically to obtain thirty samples. All teeth were painted with an acid-protective varnish, leaving a 2 mm × 4 mm window on the buccal or lingual surface depending on the section. The 2 mm × 4 mm window created an area of enamel where the brackets would bond, and there would be no etching of adjacent enamel that could lead to enhancement of demineralization. Canine and premolar orthodontic stainless steel twin brackets (Ortho Classic, McMinnville, OR) were bonded to the exposed enamel. The exposed enamel was etched with 35% phosphoric acid for 20 s and rinsed and dried. Assure (Reliance Orthodontic Products, Itasca, IL, USA) was applied to the etched surface using a microbrush and light cured for 30 s. Group 1 included fifteen samples and was bonded with Transbond XT (3M Unitek, Monrovia, CA, USA) while Group 2 included the other fifteen samples and was bonded with ACTIVA according to both manufacturers’ instructions. For each group, the bonding agent was applied to the mesh pad of the bracket and placed on the 2 mm × 4 mm window, with excess removed.
Inhibition of demineralization adjacent to the bracket was evaluated by removing 0.5 mm × 4 mm of the varnish occlusal to the bracket. Artificial caries solution consisting of 2.2 mM Ca+2, 2.2 mM PO4−3, and 50 mM acetic acid at pH 4.5 was used to immerse the samples in two separate beakers, one with Group 1 and the other with Group 2. After 3 days, the samples were removed and demineralization was detected by visualization of white chalky enamel. The teeth were then stored in deionized water until bracket removal and sectioning.
Brackets were removed and a hard tissue microtome was used to section the teeth which were buccolingually along the long axis of the tooth. One hundred micrometer sections were made through the bonding agent and the adjacent carious lesion. The sections were photographed under a polarized light microscope, and the area of demineralization was measured with a computer imagining system (Image-Pro Plus version 4.0).
Results
Thirteen teeth suffered catastrophic blowouts during sectioning leaving n = 8 for the ACTIVA group and n = 9 for the control group. The mean (±standard deviation) area (μm2) of demineralization occlusal to the bracket was 42,081 μm2 ± 33,412 for the control and 1306 μm2 ± 3694 for ACTIVA. There is a statistically significant difference (P ≤ 0.001) between the two groups, and according to the Mann–Whitney rank sum test, ACTIVA had significantly less enamel demineralization adjacent to the bracket when compared to the control. The data collected are summarized in Table 1 and Figure 1. Photographs of representative lesions are shown in Figures 2 and 3.
| Bonding agent | n | Mean(μm2)±SD | Minimum | Maximum |
|---|---|---|---|---|
| Transbond XT | 9 | 42,081±33,412 | 15,880 | 126,763 |
| Activa | 8 | 1306±3694 | 0 | 10,448 |
SD – Standard deviation
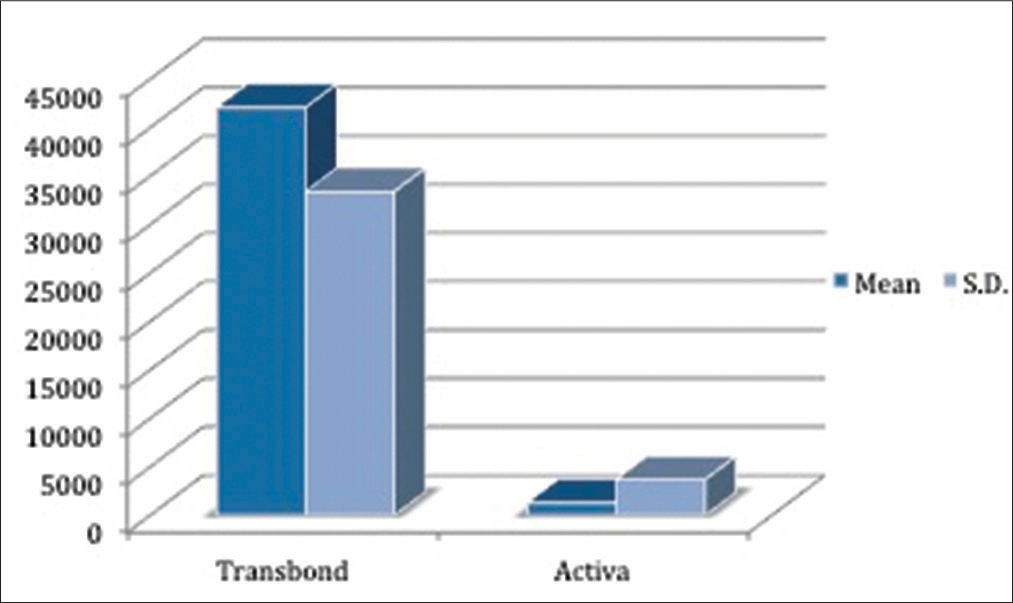
- Mean area (μm2) and standard deviation of enamel demineralization adjacent to bonding agent
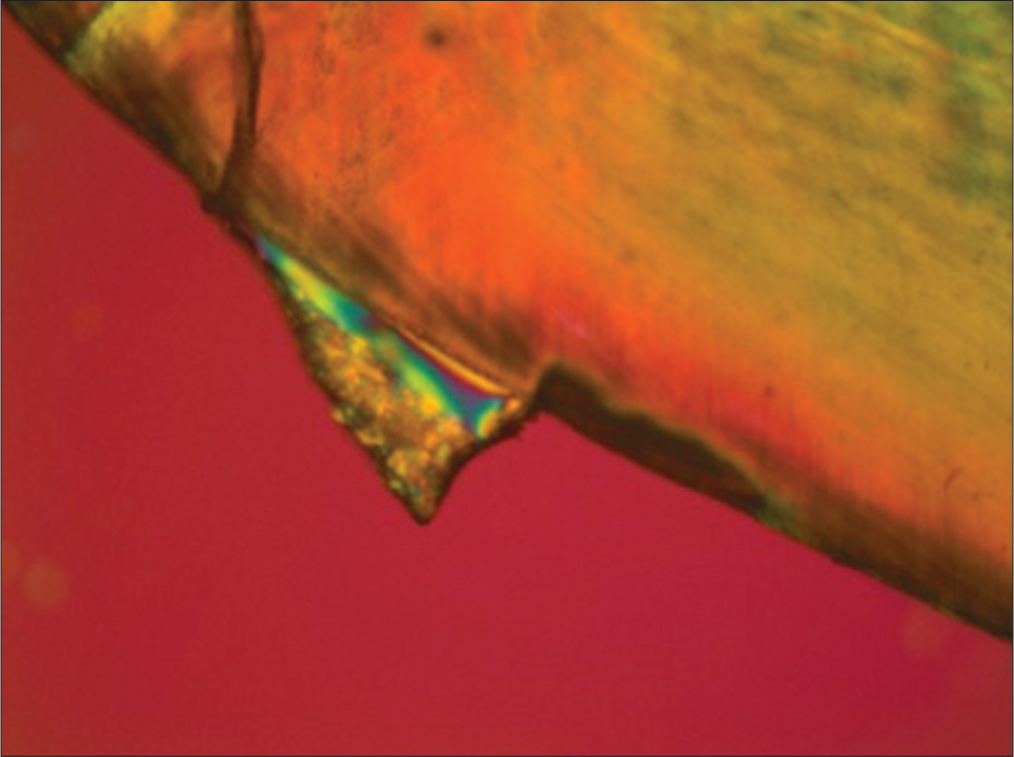
- Representative lesion of the control group (Transbond XT) under polarized light microscopy
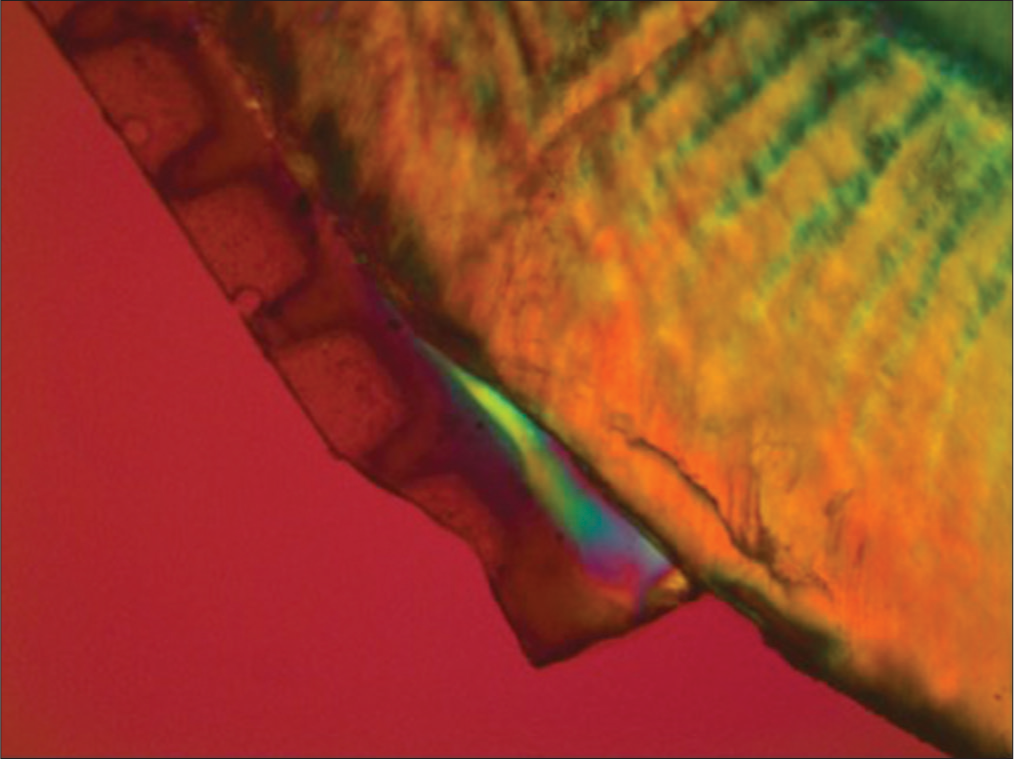
- Representative lesion of ACTIVA under polarized light microscopy
Discussion
This study demonstrated results that are coincident with other studies that fluoride-releasing bonding agents show an ability to inhibit enamel demineralization adjacent to that bonding agent when used for bonding brackets.[16-21] This proves to be beneficial at the bonding appointment, especially for an orthodontic patient that exhibits poor oral hygiene and noncompliance.
It is extremely hard to achieve total remineralization after WSLs develop, so it would be best to prevent the demineralization. ACTIVA is a bioactive composite that releases calcium, phosphate, and most importantly fluoride. A continuous release of fluoride from the bonding agent would be beneficial in prevention of WSLs. In the oral cavity, the presence of fluoride decreases the development of WSLs in three ways: inhibition of demineralization of enamel, increase in the remineralization of enamel, and the inhibition of the bacterial enzyme producers of acids.[25] Fluoride release has been shown to be the highest in the first 24 h,[26] and constant supply of low levels of fluoride in the biofilm, saliva, and dental interface is considered to be the most beneficial in preventing dental caries.[27]
If prevention does not work and WSLs develop, numerous therapies exist in the literature. Recommendations are made for the most conservative approach first before resorting to more invasive approaches. Conservatively, first, the practitioner should begin with low levels of fluoride application, then tooth whitening to camouflage WSL, and then microabrasion and finally would be a resin-based composite restoration or veneer.[28]
Obviously, prevention would be the ideal protocol and ACTIVA is shown in this study to significantly reduce enamel demineralization adjacent to orthodontic-fixed appliances. The loss of samples in this study was potentially due to the brackets being bonded too far occlusally, increasing the risk for blowouts during sectioning. A better protocol in this study would have been to bond the brackets 2 mm or even 3 mm away from the occlusal instead of 1 mm. Future studies could include this bonding technique to have more samples. Other studies could be detection of fluoride levels and release over time of ACTIVA, the remineralization effects of ACTIVA if used once WSLs are detected, and the bond strength of ACTIVA with orthodontic brackets.
Conclusions
The results of this study have demonstrated that ACTIVA, a fluoride-releasing bioactive resin-modified glass ionomer cement, inhibits demineralization of enamel adjacent to orthodontic brackets when compared to a nonfluoride-releasing control. The use of ACTIVA at the bonding appointment is a potential improvement for inhibiting WSLs throughout orthodontic treatment. Future studies are needed to determine the long-term benefits of ACTIVA, the adequacy of bond strength, and the possibility of reversal of WSLs.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- The incidence of caries and white spot lesions in orthodontically treated adolescents with a comprehensive caries prophylactic regimen – A prospective study. Eur J Orthod. 2012;34:633-9.
- [CrossRef] [PubMed] [Google Scholar]
- Enamel demineralization following orthodontic treatment. Am J Orthod. 1982;82:62-7.
- [CrossRef] [Google Scholar]
- Incidence of white spot formation after bonding and banding. Am J Orthod. 1982;81:93-8.
- [CrossRef] [Google Scholar]
- Orthodontic appliances and enamel demineralization. Part 1. Lesion development. Am J Orthod Dentofacial Orthop. 1988;94:68-73.
- [CrossRef] [Google Scholar]
- Prevalence of white spot lesion formation during orthodontic treatment. Angle Orthod. 2013;83:641-7.
- [Google Scholar]
- Plaque distribution on bonded brackets: A scanning microscope study. Am J Orthod. 1979;75:667-77.
- [CrossRef] [Google Scholar]
- Bacterial colonization associated with fixed orthodontic appliances. A scanning electron microscopy study. Eur J Orthod. 2001;23:475-84.
- [CrossRef] [Google Scholar]
- Salivary Streptococcus mutans levels in patients before, during, and after orthodontic treatment. Am J Orthod Dentofacial Orthop. 1991;100:35-7.
- [Google Scholar]
- A study of the effects of orthodontic appliances on the oral microbial flora. Oral Surg Oral Med Oral Pathol. 1964;17:658-67.
- [CrossRef] [Google Scholar]
- Effect of fixed orthodontic treatment on salivary flow, pH and microbial count. J Dent (Tehran). 2016;13:18-22.
- [CrossRef] [Google Scholar]
- Effect of a fluoride varnish on demineralization adjacent to orthodontic brackets. Am J Orthod Dentofacial Orthop. 1999;116:159-67.
- [CrossRef] [Google Scholar]
- The efficacy of a fluoride varnish in reducing enamel demineralization adjacent to orthodontic brackets: An in vitro study. Orthod Craniofac Res. 2004;7:205-10.
- [CrossRef] [PubMed] [Google Scholar]
- Prevention of demineralization around orthodontic brackets using two different fluoride varnishes. Eur J Dent. 2013;7:41-7.
- [Google Scholar]
- Effectiveness of high-fluoride toothpaste on enamel demineralization during orthodontic treatment-a multicenter randomized controlled trial. Eur J Orthod. 2014;36:678-82.
- [CrossRef] [Google Scholar]
- A prospective, randomized placebo-controlled clinical trial on the effects of a fluoride rinse on white spot lesion development and bleeding in orthodontic patients. Eur J Oral Sci. 2015;123:186-93.
- [CrossRef] [PubMed] [Google Scholar]
- Enamel demineralization adjacent to orthodontic brackets bonded with hybrid glass ionomer cements: An in vitro study. Am J Orthod Dentofacial Orthop. 1998;114:668-74.
- [Google Scholar]
- Demineralization around orthodontic brackets bonded with resin-modified glass ionomer cement and fluoride-releasing resin composite. Pediatr Dent. 2001;23:255-9.
- [Google Scholar]
- In vivo effect of a resin-modified glass ionomer cement on enamel demineralization around orthodontic brackets. Am J Orthod Dentofacial Orthop. 2004;125:36-41.
- [CrossRef] [Google Scholar]
- Effects of bonding materials on the mechanical properties of enamel around orthodontic brackets. Angle Orthod. 2012;82:187-95.
- [Google Scholar]
- Prevention of demineralization around orthodontic brackets in vitro. Am J Orthod Dentofacial Orthop. 2007;131(705):e1-9.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of fluoride varnish on demineralization adjacent to brackets bonded with RMGI cement. Am J Orthod Dentofacial Orthop. 2002;122:125-34.
- [Google Scholar]
- Decalcification and bond failure: A comparison of a glass ionomer and a composite resin bonding system in vivo. Am J Orthod Dentofacial Orthop. 1999;116:518-21.
- [Google Scholar]
- Flexural strength and flexural fatigue properties of resin-modified glass ionomers. J Clin Dent. 2015;26:23-7.
- [CrossRef] [Google Scholar]
- Comparison of mechanical properties of dental restorative material. J Dent Res. 2014;93A:1163.
- [Google Scholar]
- Therapies for white spot lesions – A systematic review. J Evid Based Dent Pract. 2017;17:23-38.
- [Google Scholar]
- Fluoride released from orthodontic bonding agents alters the enamel surface and inhibits enamel demineralization in vitro. Am J Orthod Dentofacial Orthop. 1996;109:466-72.
- [Google Scholar]
- The cariostatic mechanisms of fluoride. Acta Med Acad. 2013;42:179-88.
- [CrossRef] [PubMed] [Google Scholar]
- White spot lesions: Formation, prevention, and treatment. Sem in Orthod. 2008;14:174-82.
- [CrossRef] [Google Scholar]




